One of the uses of the drug ibuprofen, a popular non-steroidal anti-inflammatory agent, is for acute pain - for which a rapid onset of action is essential. The slow dissolution of ibuprofen in the stomach prompted the development of the more soluble ibuprofen lysinate. Pharmacokinetic investigations thus demonstrated that peak plasma concentrations are reached more rapidly, which is an important prerequisite for a fast onset of action [1]. The analgesic effects of ibuprofen and ibuprofen lysinate were compared in a recently published clinical study, the results of which now shed a different light on the pharmacokinetic advantages of ibuprofen lysinate.
Tagasi lehele Ülevaade
Riik: Eesti
Eesti
EestiKeel:eesti
Treatment of acute pain: comparison of the efficacy of ibuprofen lysinate and ibuprofen
Ibuprofen is a popular and widely used non-steroidal anti-inflammatory drug that is used for the treatment of acute mild to moderate pain. As an acid, ibuprofen dissolves slowly in the acidic environment of the stomach, so that peak plasma levels are sometimes not reached until 90 minutes after ingestion. Since a rapid onset of action is essential for the treatment of acute pain, new formulations have been developed to enable faster absorption and hence a more rapid oral bioavailability. They include effervescent tablets, liquid preparations or lysine and arginine salts of ibuprofen acid. Peak plasma concentrations are reportedly achieved with these new formulations as early as 29 to 40 minutes after ingestion. However, these values typically relate to ingestion on an empty stomach after a fast of more than 10 hours.
To date, little data on the direct comparison between ibuprofen and ibuprofen lysinate
A meta-analysis published in 2014 showed that fast-dissolving ibuprofen was more effective than usual ibuprofen [2]. However, this meta-analysis was mainly based on a small number of studies that had been carried out with ibuprofen arginate and none of the efficacy studies had used ibuprofen lysinate as comparator. The present study therefore describes the analgesic effect and onset of action of ibuprofen and ibuprofen lysinate in patients following an operation to remove wisdom teeth. The surgical removal of wisdom teeth is particularly suitable as a pain model for evaluating the efficacy of non-steroidal anti-inflammatory drugs and is recommended by the European drug regulatory authorities for the investigation of analgesics in acute somatic pain. This is because the operation is a standardised surgical procedure that only requires local anaesthesia, and which results in substantial postoperative pain that can last for up to 48 hours after the procedure.
Clinical study compared ibuprofen and ibuprofen lysinate in acute pain
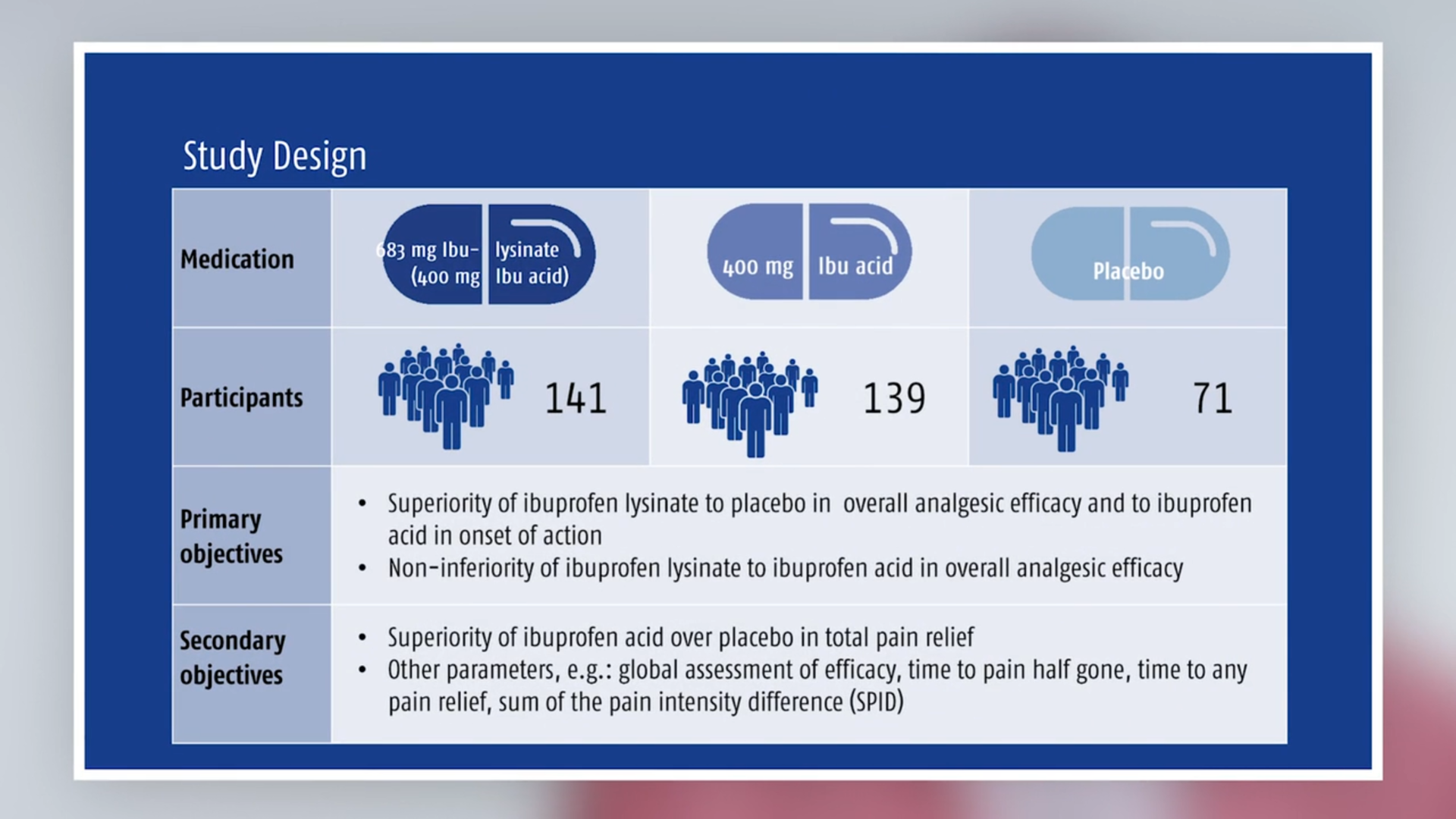
Adults aged between 18 and 60 years of age who were undergoing extraction of one or more wisdom (third molar) teeth were enrolled in the randomised, placebo-controlled, multicentre, double-blind study. They were randomly assigned in a ratio of 2:2:1 to ibuprofen lysinate (683 mg, equivalent to 400 mg ibuprofen), ibuprofen (400 mg) or placebo. Patients received a single dose of the respective drug or placebo after the effect of the local anaesthetic had worn off. The pain reduction (pain relief, abbreviated to PAR) was reported by the patients on a 5-point scale (0 = no pain relief up to 4 = complete relief of pain). The intensity of pain was recorded on a 100 mm visual analogue scale. Both parameters were each recorded successively over a period from 15 minutes to 6 hours after administration. The primary measure for efficacy was the averaged sum of the PAR scores after 6 hours (TOTPAR). Three primary hypotheses were tested (1) ibuprofen lysinate is superior to placebo in overall analgesic efficacy; (2) ibuprofen lysinate is non-inferior to ibuprofen acid (the active comparator) in overall analgesic efficacy; and (3) ibuprofen lysinate is superior to ibuprofen acid in the onset of action. The onset of action and side effects were also recorded.

Fig. 1: Pain relief over 6 hours. Figure modified from [1]

Fig. 2: Pain intensity difference over 6 hours. Figure modified from [1]
Ibuprofen lysinate not superior
Of the 351 patients enrolled in the study, 141 received ibuprofen lysinate, 139 ibuprofen and 71 placebo. In comparison with the placebo, both drugs significantly reduced pain 15 minutes after ingestion and throughout the entire period of 6 hours. The TOTPAR in the ibuprofen lysinate group was 19.57 compared to 19.96 in the ibuprofen group and 8.27 with placebo. Ibuprofen lysinate was indeed significantly more effective than the placebo (hypothesis 1), and its effect was comparable to that of ibuprofen (hypothesis 2; see Figures). The third hypothesis was rejected: ibuprofen lysinate was not superior to ibuprofen in the onset of action. This was also confirmed by the secondary endpoints investigating the onset of action (Table). Both drugs were well tolerated. All side effects (adverse events) were mild to moderate. The study therefore showed that ibuprofen lysinate was comparably effective as ibuprofen, but it was not shown that ibuprofen lysinate acted faster.

Alternatives for a faster onset of action of ibuprofen
As already mentioned, modern ibuprofen preparations such as effervescent tablets, liquid capsules or ibuprofen lysinate certainly show a faster bioavailability, but this generally requires ingestion on a fasting stomach after about 10 hours without food.
So how might a faster and more pronounced effect of ibuprofen be achieved? One possibility is the combination with caffeine. Caffeine, as a co-analgesic, can contribute to more effective pain relief. In one clinical study, the combination of 400 mg ibuprofen with 100 mg caffeine showed a more marked and faster effect than ibuprofen alone [3]. Hence the combination of ibuprofen with caffeine can be a more effective way to improve analgesia than an ibuprofen lysinate formulation.
Literature
- Kyselovič J et al. A Randomized, Double-Blind, Placebo-Controlled Trial of Ibuprofen Lysinate in Comparison to Ibuprofen Acid for Acute Postoperative Dental Pain. Pain Ther, 2020, https://doi.org/10.1007/s40122-019-00148-1.
- Moore RA et al. Faster, higher, stronger? Evidence for formulation and efficacy for ibuprofen in acute pain. Pain. 2014;155:14–21.
- Weiser T et al. Efficacy and safety of a fixed-dose combination of ibuprofen and caffeine in the management of moderate to severe dental pain after third molar extraction. Eur J Pain. 2018;22:28–38.
Conflict of interest: T. Weiser is an employee of Sanofi.
Disclosure: Medical writing and publication funded by Sanofi Aventis Deutschland GmbH.
